Cardiomyopathy: A Closer Look at the Disease
Submitted by Brianne Gallagher, RN, BSN, CCRN
Tags: cardiac arrest cardiomyopathy disease heart disease treatment

Written by Cherrie Deguzman, Heather Miller, & Brianne Gallagher
Introduction
Heart disease is a wide term used for a variety of diseases that affect the heart. Heart disease is the leading cause of death in the United States. Cardiomyopathy is one of the types of heart disease that affects about 50,000 Americans annually.
There are four types of cardiomyopathy: dilated, hypertrophic, restrictive, and arrhythmogenic right ventricular dysplasia (National Heart Lung and Blood Institute, 2007). This article will detail the different types of cardiomyopathy as well as the causes, treatment, sign and symptoms, diagnostic procedures and prevention. It will also cover ways to live with cardiomyopathy and end of life care.
Cardiomyopathy is a disease of the muscles of the heart. It can be broken down into primary and secondary classifications. In primary cardiomyopathy, the disease can’t be related to a specific cause. In secondary cardiomyopathy it is related to a cause such as hypertension, disease of the heart valves, arterial diseases, or a congenital condition (American Heart Association, 2007).
In cardiomyopathy, the myocardium becomes inflamed and enlarged and doesn’t function as properly as it should. The heart becomes weaker as the disease worsens which makes it more difficult to pump blood to the rest of the body. This, in turn, can lead to more complications such as heart failure, abnormal heart rhythms, swelling from fluid build up in the hands, ankles, and feet, backup of fluid in the lungs, and many other complications (National Heart Lung and Blood Institute, 2007).
Dilated Cardiomyopathy
The most common form of cardiomyopathy is dilated. It usually affects more males than females, and those between the ages of 20-60. Dilated cardiomyopathy affects the ventricles of the heart and the atria, usually starting in the left ventricle. The heart muscle starts to stretch and becomes thinner which causes the inside of the ventricle to become enlarged. As the disease progresses, it starts to affect the right ventricle and then the atria becomes affected (National Heart Lung and Blood Institute, 2007).
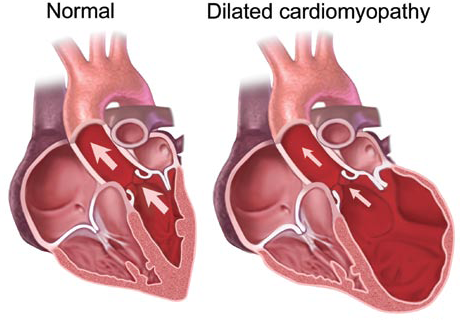
Blood flow slows as it goes through an enlarged heart causing blood clots to form which can then travel to the lungs, brain, coronary arteries, or many other areas of the body, which can lead to further complications (Understanding Cardiomyopathy, 2004). It also can cause heart valve problems, heart arrhythmias, as well as many other conditions (National Heart Lung and Blood Institute, 2007).
Treatment for dilated cardiomyopathy may consist of blood thinners to reduce clot formation, antiarrhythmic medications and in advanced conditions a heart transplant may be needed (American Heart Association, 2007).
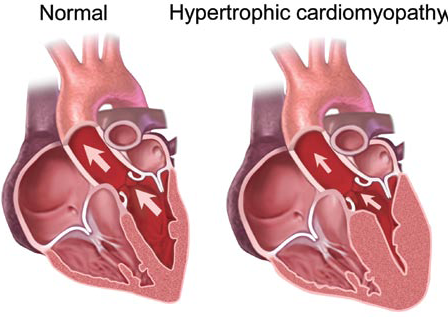
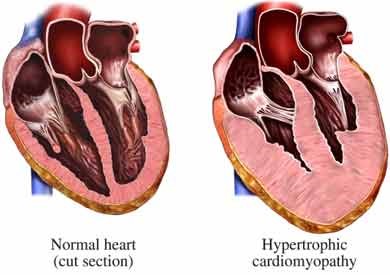
Hypertrophic Cardiomyopathy
Hypertrophic cardiomyopathy differs from dilated because in hypertrophic the muscle itself enlarges, especially the septum. This is usually caused by a genetic condition. The thickness of the muscle decreases the ventricular chamber size and causes them to take a longer time to relax.
It also makes blood filling more difficult during diastole, thus making the heart more dependent on the atrial contraction for filling. Increase in septal size can cause certain muscles in the heart to misalign causing the mitral valve to obstruct blood flow to the aorta from the left ventricle during contraction (Understanding Cardiomyopathy, 2004).
Treatment for hypertrophic cardiomyopathy may consist of different types of medications such as beta blockers, calcium channel blockers, or antiarrhythmic medications if needed. If drug treatment fails, surgical treatment may be possible to remove the obstructive form.
A nonsurgical treatment is alcohol septal ablation (ASA). It involves injecting alcohol along a branch of one of the coronary arteries to necrose the extra muscle allowing the myocardium to thin out without surgical treatment (American Heart Association, 2007). ASA in selected patients has been demonstrated to be safe and effective, and with very low risk of complications. Furthermore, it continues its effects in improving symptoms years after the initial procedure.
Restrictive Cardiomyopathy
One of the less common types of cardiomyopathy is restrictive. It usually affects the older adult population. In this type the ventricles become stiff and rigid because the normal heart muscle has been replaced by an abnormal tissue which is usually scar tissue (National Heart Lung and Blood Institute, 2007).
This abnormal tissue impairs the ventricles from stretching and filling properly. A person with this type of cardiomyopathy usually complains of heart failure symptoms such as being tired. They also may have swollen hands or feet and difficulty breathing with activity (American Heart Association, 2007).
Since restrictive cardiomyopathy is less common, not as much is known about its pathology. It has been linked to types of infiltrative disease such as amyloidosis and connective tissue disorders (Understanding Cardiomyopathy, 2004). For nurses working with patients who present with cardiac symptoms, understanding the nuances of cardiomyopathy signs, symptoms, and the registered nurse's role is essential.
Arrhythmogenic Right Ventricular Dysplasia
A rare type of cardiomyopathy is arrhythmogenic right ventricular dysplasia. It is thought to be an inherited disease that usually affects teenagers or young adults. It occurs when the right ventricle muscle dies and is replaced by scar tissue. This causes electrical problems in the hearts conduction system leading to arrhythmias.
The usual complaint is feeling a strong, irregular heartbeat and often passing out after exercise or physical activity. This type is often the cause of young athletes dying with “sudden cardiac death” (National Heart Lung and Blood Institute, 2007). Apoptosis (programmed cell death) is thought to be one of the causes of arrhythmogenic right ventricular dysplasia. Why the right ventricle is mainly involved is unknown. In late disease the left ventricle may become involved and this has a very poor prognosis (health-cares.net, 2005).
Causes of Cardiomyopathy
The cause of cardiomyopathy is not always known. Most of the time that is the case with children with cardiomyopathy. It can be passed down through family members or it can also be caused by other diseases or conditions.
Dilated cardiomyopathy can be inherited or it can also be caused by another source such as: heart attacks, coronary artery disease, infections of the heart, excessive alcohol consumption, complications during pregnancy, toxins, cocaine and amphetamine use, diabetes, and thyroid disease.
The cause of hypertrophic cardiomyopathy is often unknown but it can be inherited or can develop due to hypertension or even aging. Restrictive cardiomyopathy is caused by certain diseases or conditions, including: Hemochromatosis which is deposits of iron that are increased in tissues, amyloidosis, sarcoidosis, and connective tissue disorders. It is thought that arrhythmogenic right ventricular dysplasia is strictly inherited (National Heart Lung and Blood Institute, 2007).
A person of any age can develop cardiomyopathy, however, dilated cardiomyopathy is more likely to develop in African Americans and in men (Understanding Cardiomyopathy, 2004). Arrhythmogenic right ventricular dysplasia is more prominent in teen and young adults than older individuals.
Signs, Symptoms, and Diagnosis
Many people with cardiomyopathy have no symptoms. As the disease worsens usual signs and symptoms include: tiredness, weakness, dyspnea with activity or even rest, and edema in the abdomen, legs, ankles, and feet. Other symptoms include lightheadedness, arrhythmias, and heart murmurs (National Heart Lung and Blood Institute, 2007).
Diagnosis of cardiomyopathy is made by a person’s medical and family history, physical exam, and diagnostic tests and procedures. The most common diagnostic testing is an electrocardiogram better known as an ECG. This test can detect arrhythmias by measuring the rate and regularity of a person’s heartbeat.
Another common test is an echocardiogram. This looks at the size and shape of the heart as well as how well the chambers and valves are functioning. Chest x-rays and MRI’s can also show enlarging of the heart muscles. Usually more than one test is needed to make a positive diagnosis. If a doctor still suspects cardiomyopathy and these tests don’t show it further testing can be done (National Heart Lung and Blood Institute, 2007). Nurses play a vital role in applying critical thinking skills during the diagnostic workup to catch subtle signs early.
Invasive testing for cardiomyopathy is another option for diagnosis. Cardiac catheterization is a type of invasive diagnostic testing that can be done. In this test doctors can check the pressure and blood flow throughout the different chambers of the heart. They can also view the arteries of the heart.
Coronary angiography is done with the cardiac catheterization which allows the physician to view the flow of blood to the myocardium. A dye is also injected into the different chambers to evaluate how effectively the heart is pumping. A myocardial biopsy of the heart wall tissue may help distinguish between the different types of cardiomyopathy (National Heart Lung and Blood Institute, 2007).
Treatment Options
Treatment of cardiomyopathy varies from patient to patient. Not everyone with cardiomyopathy needs treatment. Treatment is also dependent on the type of cardiomyopathy the patient has. The main goal of treatment is to manage the condition and control the symptoms and try to stop the disease from worsening.
Medication treatment is usually the first step. There are a vast selection of medications ranging from diuretics, beta blockers, and antiarrhythmics, to anticoagulants, antibiotics, and steroids. Beta-blocker medicines and calcium antagonist medicines are the mainstay of treatment. These can slow the heart rate, make the heart contract less forcefully, and can allow more time for the ventricle to fill each heartbeat. These medicines may be used to treat chest pain, breathlessness and palpitations (National Heart Lung and Blood Institute, 2007).
Different surgical treatments are used for different types of cardiomyopathy. One of the surgical treatments involves removing part of the thickened muscle in hypertrophic cardiomyopathy. Physicians can also implant a pacemaker to help control patient arrhythmias or use a left ventricular assist device to help pump blood to the body. An implanted defibrillator can be used to treat lethal arrhythmias and ideally prevent sudden cardiac death. In very progressive cardiomyopathy a heart transplant can be done (National Heart Lung and Blood Institute, 2007). For patients managing cardiac conditions at home, digital technology tools for heart failure can support ongoing monitoring and adherence.
Lifestyle Changes and Living with Cardiomyopathy
Lifestyle changes can also be made to reduce symptoms and progression of the disease. They can also be used to help prevent cardiomyopathy. The most common change would be to quit smoking, lose excess weight, and avoid alcohol. Other changes would be reducing sodium intake, exercising, decreasing stress, and treating the underlying condition such as hypertension or diabetes (National Heart Lung and Blood Institute, 2007).
Cardiomyopathy differs from other types of heart disease in many ways. It is the leading cause of heart transplants. Many people live with cardiomyopathy for years without any treatment. While some with cardiomyopathy may have serious complications and symptoms, it is possible to live a healthy, active life with cardiomyopathy without any problems or symptoms.
Ways to help improve a patient’s quality of life if they already have cardiomyopathy include taking your medications as prescribed, make the necessary lifestyle changes, and seeing their doctor regularly. It may also be necessary to take prophylactic antibiotics to help prevent infections of the heart in certain conditions (National Heart Lung and Blood Institute, 2007).
Those with cardiomyopathy should also be aware of the signs and symptoms of progression of the disease and notify the doctor if any new symptoms occur. It is also important to discuss what types of exercise are appropriate and those to avoid. Diet is another area that should be addressed with a physician.
Some types of cardiomyopathy require extra intake of fluid and also restriction of other things such as salt and fat. Since cardiomyopathy often runs in families, it is best that all immediate members of a family to get tested periodically (National Heart Lung and Blood Institute, 2007).
End of Life Considerations
Death is more likely to occur from arrhythmogenic right ventricular dysplasia because of the sudden onset of a fatal arrhythmia. Usually death isn’t necessarily from the cardiomyopathy, but from the complications of it such as heart failure.
If heart failure is severe enough, treatments may stop working. In that case, end of life decisions need to be made and wishes need to be made known to family members. Hospice is another option in end of life care. Hospice can provide comfort and support for the patient and emotional support for the family members as well. They will work with each person individually to make the process as simple as possible (National Heart Lung and Blood Institute, 2007). Understanding whether nurses are educationally prepared for end-of-life care is an ongoing concern in the profession.
Conclusion
This article has discussed the different types of cardiomyopathy: dilated, hypertrophic, restrictive, and arrhythmogenic right ventricular dysplasia. It has also discussed the different causes, treatments, sign and symptoms, and diagnostic testing procedures. Cardiomyopathy is a growing problem. Truly more research needs to be done on certain types of cardiomyopathy. We see more and more patients with cardiomyopathy and not a lot of answers to the patient’s questions. We hope this paper has improved the understanding of cardiomyopathy so that questions can be answered.
References
- American Heart Association: Cardiomyopathy. (2007). Retrieved November 11, 2007 from http://www.americanheart.org/print_presenter.jhtml?idetifier=4468
- Health-Care’s. (2005). Retrieved November 11, 2007 from http://heart-disease.health-cares.net/cardiomyopathy-treatment.php
- National Heart Lung and Blood Institute: Cardiomyopathy Disease and Condition Index. (2007). Retrieved November 11, 2007 from http://www.nhlbi.nih.gov/health/dci/Deseases/cm/cm_all.html
- Nogic, J., et al. (2018). Alcohol Septal Ablation for Hypertrophic Obstructive Cardiomyopathy: A 16-year Australian Single Centre Experience. Heart, Lung, and Circulation, 27, 1446-1453.
- Understanding Cardiomyopathy. (2004, April). Nursing. Retrieved November 6, 2007, from Academic Search Premier Database.