Enhancing Equity and Access in Canadian Maternal Healthcare
Submitted by Shahnaz Shahid Ali, Dr. Panagiota Tryphonopoulos
Tags: canada childbirth pregnancy

Summary
The Canadian healthcare system is governed by federal principles that are provincially administered to provide universal access to maternal health services. Nevertheless, disparities exist in the system related to access in urban, rural, and indigenous communities that are driven by social determinants affecting maternal health at the individual, family, and community level, along with health system and policy-related factors. A policy focus is needed to ensure equitable access to comprehensive maternal health services in Canada.
Background
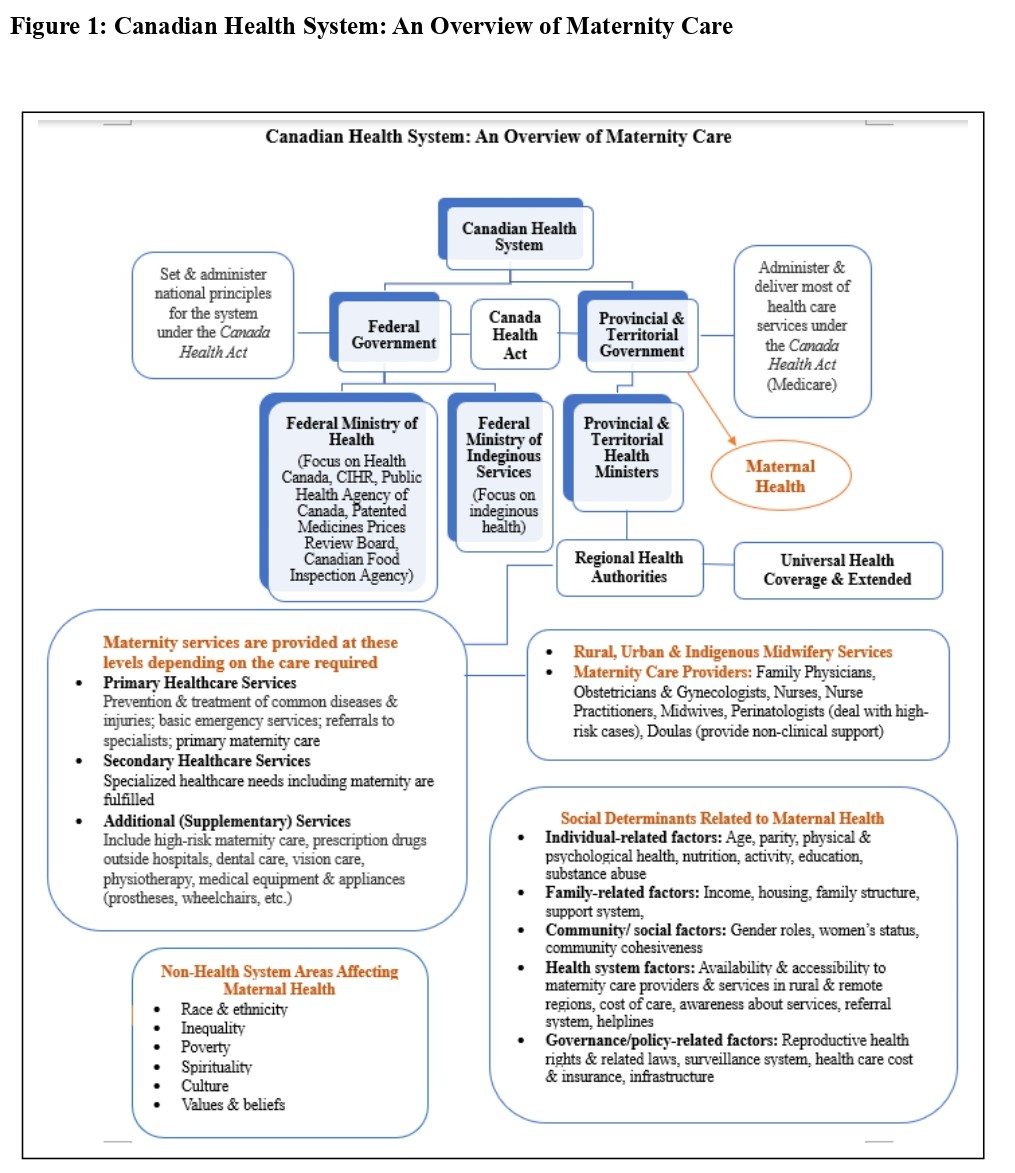
The Canadian health system applies a shared responsibility model, in which the Federal Government sets national principles through the Canada Health Act, creating the foundation of the system, and the Provincial and Territorial Governments administer and deliver services, including maternal health (Health Canada, 2015).
Midwifery services are explicitly mentioned as a key component for rural, urban, and Indigenous populations. The federal government has a specific focus on Indigenous health through Indigenous Services Canada. Maternity services are provided at primary, secondary, and additional levels based on the required needs (basic versus high-risk care) (Health Canada, 2015). A diverse range of healthcare providers, family physicians, obstetricians, perinatologists, nurses, midwives, and doulas are available to provide maternal care (see Figure 1).
The strengths of this model include universal access to maternal health services resulting in low national rates of maternal morbidity and mortality, use family-centered care approach to maternal and newborn care, acknowledging pregnancy as a normal physiological process and including the family in decision-making, and the availability diverse healthcare providers allowing women to choose care provider and birthplace and fulfill the needs of individuals at different levels.
Issues in the System
The Canadian healthcare system lays a strong foundation for maternal health, emphasizing universal health coverage (Rodriguez, 2022); however, challenges exist in terms of inequitable access to services, shortage of healthcare providers, influence of the social determinants on maternal health, and medicalization of childbirth with the use of interventions. Inequitable access to services: Significant disparities in access to pregnancy, childbirth, and afterbirth (perinatal) care exist, particularly for Indigenous women, black and other marginalized individuals, and their families (Adegoke et al., 2025), as well as those living in rural and remote areas due to structural and systemic factors in the healthcare settings. Maternal and infant mortality is high among Indigenous communities in Canada (Public Health Agency of Canada [PHAC], 2018) due to healthcare disparities (Sheppard et al., 2017). Shortage of healthcare providers: The system faces concerns regarding a shortage and unequal geographical availability of maternity care providers (HCPs). This has led to the centralization of services in some rural areas, requiring patient travel.
Due to the closure of maternity programs in rural northern Ontario, a continuous reduction in maternity care settings and care providers has led to the development of a maternity care desert, reducing access to perinatal care to individuals living in those areas (Lamb et al., 2025). According to the Canadian Association of Midwives (CAM) (2023), there is a need for 9000 additional midwives by 2030 in Canada to meet the reproductive and sexual healthcare needs of individuals. Influence of the social determinants on maternal health: The trends observed in maternal health are influenced by different factors, including the Social Determinants of Health (SDOH) (United Nations Development Programme [UNDP], 2015). The SDOH can lead to poor maternal and infant health outcomes (Malin et al., 2025). Non-health system factors like race, ethnicity, inequality, poverty, and income significantly impact maternal health outcomes, suggesting that a holistic approach addressing these social determinants is essential (Crear-Perry et al., 2021). Medicalization of childbirth: While some de-medicalization trends (e.g., lower episiotomy rates) are positive, Canada still experiences high and varying rates of interventions like caesarean births across regions. The cesarean section (C-section) rate has increased gradually, with 33.4% in 2023–2024 and 29.9% in 2019–2020 (Canadian Institute for Health Information [CIHI], 2025). The interventions may not always be evidence-based or based on medical need; however, often related to the trust in technology instead of the natural physiological childbirth processes (Rivard & Gagnon, 2025).
Recommendations
To address the issues in the healthcare system and ensure the provision of high-quality maternal health services across Canada, the following recommendations are proposed:
- Invest in Rural and Remote Services: Increase funding and incentives to recruit and retain maternity care providers (midwives, nurses, physicians) in underserved rural and remote regions to improve accessibility. For example, British Columbia has extended its Provincial Recruitment and Retention Incentives program for healthcare workers in 76 rural communities until March 31, 2026. Likewise, Ontario offers the Northern and Rural Recruitment and Retention Initiative, providing taxable grants of up to $125,000 to eligible physicians who commit to a full-time practice in underserved areas over the past four years (Ministry of Health, 2024). Similar initiatives can be led across Canada to strengthen maternal healthcare.
- Support Indigenous and Marginalized Communities' Health Care: Prioritize funding and recognition for Indigenous and marginalized midwifery services and culturally safe care models, supporting self-determination in health services. Such strategies can play an important role in minimizing intergenerational trauma among Indigenous communities and acknowledge language, documentation, and access to primary care among marginalized communities. In 2024-25, the government launched the $2 billion Indigenous Health Equity Fund, an investment over 10 years to improve access to quality and culturally safe health services for First Nations, Inuit, and Métis health priorities initiatives (Indigenous Services Canada, 2024). Similar initiatives should also be considered for marginalized communities living in Canada.
- Address the Structural and Social Determinants of Health: Acknowledge the non-health system factors impacting maternal health outcomes by implementing policies to tackle the factors, like housing stability, poverty reduction, and income inequality.
- Enhance Awareness and Referral Systems: Improve public awareness campaigns about available services and refine referral systems to ensure seamless transitions between primary, secondary, and additional care levels, regardless of location or background.
- Invest in the Development of Healthcare Providers: Offer funding, scholarships, and grants to provide equitable opportunities for domestic and international individuals aiming to pursue a professional healthcare degree or get through bridging programs and serve the community by meeting the healthcare needs of people.
- Acknowledge the Physiological Process of Childbirth: Provide awareness at all levels about normality in childbirth, and the need for immediate interventions in high-risk cases. For almost 20 years now, the Canada Prenatal Nutrition Program (CPNP) has been promoting breastfeeding among vulnerable populations. This community-based approach helps service providers work together to influence wider community initiatives (PHAC, 2014). Similar social campaigns can be facilitated to provide awareness and minimize misinformation. Implementing these policies will move the Canadian health system toward a more equitable and effective model of maternal care for all its citizens.
Conclusion
The Canadian health system provides good basic care, but ongoing efforts are needed to ensure that high-quality, equitable, and accessible culturally safe maternal care is available across the country.
Figure 1: Canadian Health System: An Overview of Maternity Care
References
- Adegoke, K., Adegoke, A., Dawodu, D., & Kayode, T. (2025). Systemic racism in Canadian healthcare: A policy and equity analysis. Journal of Primary Care & Community Health, 16, 21501319251386672. https://doi.org/10.1177/21501319251386672
- Canadian Association of Midwives [CAM]. (2023). New position statement: The enabling environment for midwifery in Canada. https://canadianmidwives.org/sites/canadianmidwives.org/wp- content/uploads/2023/06/PositionStatement_CAMPS_EnablingEnvironment_VD_20230622.pdf
- Canadian Institute for Health Information [CIHI]. (2025). Hospital stays in Canada, 2023–2024.
- Crear-Perry, J., Correa-de-Araujo, R., Lewis Johnson, T., McLemore, M. R., Neilson, E., & Wallace, M. (2021). Social and structural determinants of health inequities in maternal health. Journal of Women's Health, 30(2), 230–235. https://doi.org/10.1089/jwh.2020.8882 Health Canada. (2015).
- Canada Health Act: Annual Report 2015-2016. Government of Canada. www.canada.ca Indigenous Services Canada. (2024, August 9). Indigenous health equity fund. Government of Canada. https://www.sac-isc.gc.ca/eng/1721758041536/1721758068269 Lamb, I. R., Dumonski, N. A., Corneil, H.,
- Mensour, C. C. M., & Orrantia, E. (2025). Understanding the maternity care desert: A qualitative study on factors contributing to the closure of obstetrical programmes in rural northern Ontario. Canadian Journal of Rural Medicine: The Official Journal of the Society of Rural Physicians of Canada, 30(2), 79–88. https://doi.org/10.4103/cjrm.cjrm_49_24
- Malin, K. J., Vance, A. J., Moser, S. E., Zemlak, J., Edwards, C., White-Traut, R., Koerner, R., McGrath, J., & McGlothen-Bell, K. (2025). The impact of social determinants of health on infant and maternal health using a reproductive justice lens. BMC Pregnancy and Childbirth, 25(1), 577. https://doi.org/10.1186/s12884-025-07693-y Ministry of Health. (2024, January 15). Northern and rural recruitment and retention initiative. Government of Ontario. https://www.ontario.ca/document/northern-health-programs/northern-and-rural-recruitment-and-retention-initiative
- Public Health Agency of Canada. (PHAC). (2018). Key health inequalities in Canada: A national portrait. Ottawa: Public Health Agency of Canada.
- Public Health Agency of Canada. (PHAC). (2014). Protecting, promoting, and supporting breastfeeding: A practical workbook for community-based programs. Government of Canada. https://www.canada.ca/en/public-health/services/publications/healthy-living/protecting-promoting-supporting-breastfeeding.html
- Rivard, A. & Gagnon, R. (2025). A century of change: The medicalization of birth in Quebec. Your body, your birth, your choice. https://enfantement.org/en/community/real-voices/a-century-of-change-the-medicalization-of-birth-in-quebec/ Rodriguez, E. (2022). Is Canadian healthcare truly universal? Health inequities based on immigration status. Citizens for Public Justice. https://cpj.ca/is-canadian-healthcare-truly-universal-health-inequities-based-on-immigration-status/
- Sheppard, A. J., Shapiro, G. D., Bushnik, T., Wilkins, R., Perry, S., Kaufman, J. S., Yang, S., & Arbour, L. (2017). Birth outcomes among First Nations, Inuit, and Métis populations. Health Reports, 28(11), 11–16. www150.statcan.gc.ca
- United Nations Development Programme. (UNDP). (2015). A social determinants approach to maternal health. https://www.undp.org/publications/social-determinants-approach-maternal-health