Sustained Breastfeeding, When Possible: Nursing-Driven, Team-Based Care and Maternal–Infant Outcomes
Submitted by Zeena Nackerdien, PhD
Tags: assessment behavioral breastfeeding care clinical counseling health postpartum risk support

By Zeena Nackerdien, PhD
Department of Nursing, Montefiore Medical Center, Bronx, NY
Nursing-Driven Team-Based breastfeeding support, grounded in informed choice, can shape maternal-infant health outcomes.
Introduction
Leading health authorities recommend initiating breastfeeding within one hour of birth and maintaining exclusive breastfeeding for six months, followed by continued breastfeeding with complementary foods up to two years or longer (Kinshella et al., 2022; Meek & Noble, 2022; WHO, 2023). These recommendations reflect exposure‑dependent benefits that are most consistently realized with sustained exclusivity (Figure 1) (American College of Obstetricians and Gynecologists [ACOG], 2021).
In high‑resource settings, initiation rates are often strong, supported by Baby‑Friendly practices—early skin‑to‑skin, rooming‑in, and avoidance of non–medically indicated formula supplementation—yet continuation frequently falters after discharge when skilled support and clear referral pathways may be limited (ACOG, 2021; World Health Organization [WHO] & United Nations Children’s Fund [UNICEF], 2018). Equally important, facilities should organize interprofessional team-based workflows to ensure continuity beyond the hospital and reduce avoidable drop-off.
Additionally, local data indicate that Baby-Friendly practices can shape health care utilization patterns among Medicaid-insured newborns, underscoring the need for equitable access to skilled lactation care (Harrison Long, Papas, & Paul, 2023). The clinical priority should not be promotion in medically appropriate cases alone, but ongoing, nurse-delivered support across settings.
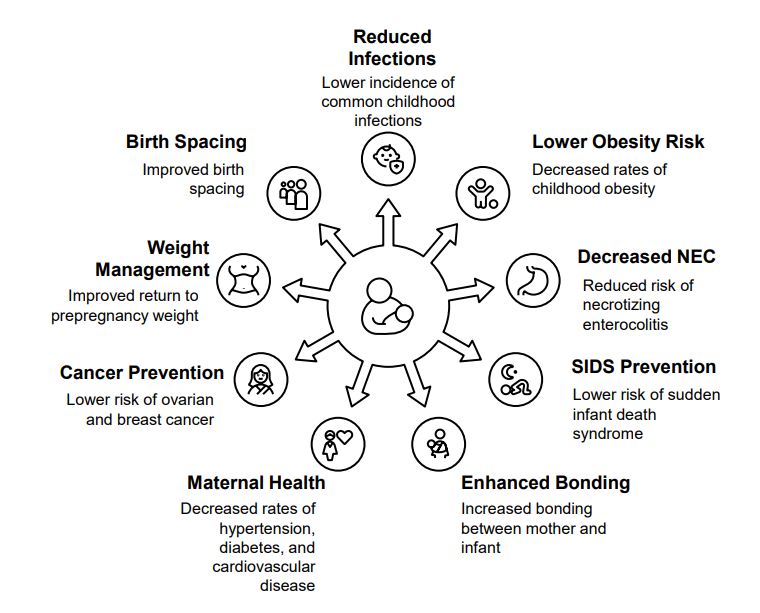
Figure 1: Benefits of Breastfeeding (ACOG, 2021)
Breastfeeding is associated with a range of short‑ and long‑term health benefits for both infants and lactating parents across diverse care settings. Infant outcomes include lower rates of common infectious illnesses, reduced risk of childhood obesity, decreased incidence of necrotizing enterocolitis, reduced risk of sudden infant death syndrome, and enhanced mother–infant bonding. Maternal outcomes include improved postpartum weight regulation, improved birth spacing, lower lifetime risk of breast and ovarian cancers, and reduced long‑term cardiometabolic risk. Professional organizations emphasize that these outcomes are optimized when breastfeeding is actively supported through evidence‑based, patient‑centered practices across the prenatal, intrapartum, and postpartum continuum of care.
Standard Exclusive Breastfeeding Definition
“Exclusive breastfeeding means only human milk, at breast or expressed; no other liquids or solids, with exceptions limited to oral rehydration solution and drops or syrups for vitamins, minerals, or medicines” (WHO, 2023; WHO & UNICEF, 2018). Using this exact wording aligns counseling and documentation and reduces confusion across handoffs (WHO & UNICEF, 2018).
Adopting this standardized definition across disciplines (nursing, medicine, lactation, WIC) improves clarity in discharge instructions and quality dashboards.
Early Feeding Challenges and Bedside Assessment
Pain, ineffective latch, delayed lactogenesis, and perceived low milk supply are common reasons for stopping exclusivity (ACOG, 2021). Nurses can mitigate these factors by directly observing a full feed, assessing position and latch quality, and documenting milk transfer rather than minutes at breast (ACOG, 2021; WHO, 2023).
When feeds are ineffective or supplementation is clinically indicated, promptly initiating hand expression or pumping protects supply and preserves a clear path back to exclusivity (WHO, 2023; WHO & UNICEF, 2018). Normalize frequent and cluster feeding, offer targeted pain management and nipple care, and respond early to parental distress. These actions build confidence, reduce avoidable supplementation, and keep care individualized and respectful (ACOG, 2021; Meek & Noble, 2022).
Where challenges persist, bedside nursing assessment should trigger timely referrals to appropriate interprofessional team members for joint problem-solving.
Consistent Messaging and Documentation
Conflicting messages undermine trust and may trigger premature cessation. Use a single counseling script anchored in the WHO definition, and maintain a supportive—not prescriptive—tone across all encounters (WHO & UNICEF, 2018; Meek & Noble, 2022). Chart two fields daily (exclusive breastfeeding since birth and exclusive breastfeeding in the last 24 hours) to clarify trajectory and improve continuity (Nanishi et al., 2023).
Interpret short recall windows cautiously. Twenty‑four–hour recall can overestimate exclusivity and should not be the only indicator on quality dashboards. Pair metrics with brief clinical notes on latch, transfer, and parental goals to retain context and avoid misclassification (Nanishi et al., 2023; WHO & UNICEF, 2018).
Align scripts and documentation across nursing, medical, and lactation teams so families hear one plan from the entire care team.
If Supplementation Is Clinically Indicated—Protect Supply and Plan the Return
Supplementation is sometimes appropriate; when introduced without a plan, it can reduce supply and shorten duration (WHO, 2023). Explain the medical rationale in plain language, begin milk expression immediately, and document type, volume, route, timing, and reassessment points to support relactation (ACOG, 2021; WHO & UNICEF, 2018).
Framing supplementation as support, rather than failure, preserves intent, reduces stigma, and keeps families engaged (WHO, 2023). Ideally, the interprofessional team should co-create the return-to-lactation plan with the parent to protect supply while honoring informed choice.
Nonjudgmental Counseling and Maternal Mental Health
Perceived pressure to breastfeed is associated with higher anxiety and depressive symptoms and can lower engagement with support services (Grattan et al., 2024). Lead with informed choice, emotional validation, and clear goal‑setting questions—e.g., “What matters most to you right now?”—to sustain engagement while honoring autonomy (Meek & Noble, 2022; Grattan et al., 2024).
Reassure families that lactation help continues regardless of feeding path, and screen or refer for mental health concerns when indicated (Meek & Noble, 2022). Embed rapid access to mental/behavioral health and social work referrals in the lactation pathway so families receive whole-person care regardless of feeding decisions.
Additionally, behavioral counseling delivered at multiple touchpoints (during pregnancy and postpartum) has a moderate net benefit for sustaining exclusivity through six months, supporting investment in scalable nurse‑delivered interventions (USPSTF, 2025).
After Discharge—Make Continuity of Support the Default
Feeding difficulties often intensify once families leave the hospital, particularly when timely follow‑up is absent or referral pathways are unclear. Treat discharge as a clinical intervention: re‑observe latch and transfer; when risk exists (weight, jaundice, hydration), protect supply and specify the supplement plan with relactation steps (WHO & UNICEF, 2018).
Schedule early follow‑up at two to four days and again around week two, provide direct lactation contact and telehealth access, and make warm handoffs—a direct, person‑to‑person transfer of care in which the nurse actively connects the family with the next provider rather than simply giving written information—to the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC), International Board-Certified Lactation Consultants (IBCLCs), and community‑based breastfeeding support programs (WHO & UNICEF, 2018; Meek & Noble, 2022).
This nurse action is based on the recognition that ongoing breastfeeding support can be delivered by an interprofessional team in and outside the hospital, as well as peers.
When to Seek Immediate Help
Seek prompt clinical evaluation for poor feeding, weight loss exceeding 7–10%, signs of dehydration, lethargy, or worsening jaundice; activate urgent mental health support for maternal distress or suicidal ideation (ACOG, 2021; Grattan et al., 2024).
Clarify which care team members to contact for urgent issues and include direct phone numbers to reduce delays.
Key Takeaway
Sustained exclusive breastfeeding is achievable when nursing practice, in partnership with an interprofessional team, integrates a common definition, real-time bedside assessment of milk transfer, respectful counseling, clearly documented supplementation plans, and reliable early follow-up. These actions align with guidance from leading authorities and can be implemented without coercion while honoring informed choice (ACOG, 2021; WHO & UNICEF, 2018; Meek & Noble, 2022; USPSTF, 2025).
This shared responsibility model avoids placing undue burden on nurses and better reflects how families receive care across hospital and community settings.
References
American College of Obstetricians and Gynecologists. (2021). Barriers to breastfeeding: Supporting initiation and continuation of breastfeeding (Committee Opinion No. 821). Obstetrics & Gynecology, 137, e54–e62. https://doi.org/10.1097/AOG.0000000000004232
Grattan, R. E., London, S. M., & Bueno, G. E. (2024). Perceived pressure to breastfeed negatively impacts postpartum mental health outcomes over time. Frontiers in Public Health, 12, 1357965. https://doi.org/10.3389/fpubh.2024.1357965
Harrison Long, C., Papas, M., & Paul, D. A. (2023). The impact of the Baby Friendly Hospital Initiative on healthcare utilization among newborns insured by Medicaid in Delaware. BMC Pediatrics, 23, 613. https://doi.org/10.1186/s12887-023-04371-9
Kinshella, M. L. W., Salimu, S., Vidler, M., et al. (2022). Beyond early initiation: Postpartum breastfeeding support challenges in Malawian hospitals. PLOS Global Public Health, 2(11), e0001266. https://doi.org/10.1371/journal.pgph.0001266
Meek, J. Y., & Noble, L.; Section on Breastfeeding, American Academy of Pediatrics. (2022). Policy statement: Breastfeeding and the use of human milk. Pediatrics, 150(1), e2022057988. https://doi.org/10.1542/peds.2022-057988
Nanishi, K., Green, J., Shibanuma, A., et al. (2023). Challenging the utility of 24-hour recall of exclusive breastfeeding in Japan. BMJ Global Health, 8, e013737. https://doi.org/10.1136/bmjgh-2023-013737
U.S. Preventive Services Task Force. (2025). Primary care behavioral counseling interventions to support breastfeeding: Recommendation statement. JAMA, 333(17), 1520–1526. https://doi.org/10.1001/jama.2025.3062
World Health Organization, & United Nations Children’s Fund. (2018). Protecting, promoting and supporting breastfeeding in facilities providing maternity and newborn services: The revised Baby Friendly Hospital Initiative. World Health Organization. https://www.who.int/publications/i/item/9789241513807
World Health Organization. (2023). Exclusive breastfeeding for optimal growth, development and health of infants. https://www.who.int/tools/elena/interventions/exclusive-breastfeeding